The FY 2027 SNF proposed rule may not be a long document, but skilled nursing operators should not mistake its size for simplicity.
CMS has proposed a 2.4% update to SNF PPS payment rates for fiscal year 2027, based on a 3.2% market basket update reduced by a 0.8% productivity adjustment. The rule also includes updates to the SNF Quality Reporting Program, future all-payer MDS reporting requirements, and a significant request for information around PDPM case mix patterns.
For operators, the biggest issue is not simply the proposed payment increase. It is what CMS is signaling about the future of reimbursement, coding, documentation, therapy utilization, and quality visibility.
In other words, the FY 2027 SNF proposed rule is not just about next year’s rates.
It is about whether your facility’s documentation, MDS coding, therapy delivery, and quality performance can stand up to increased scrutiny.
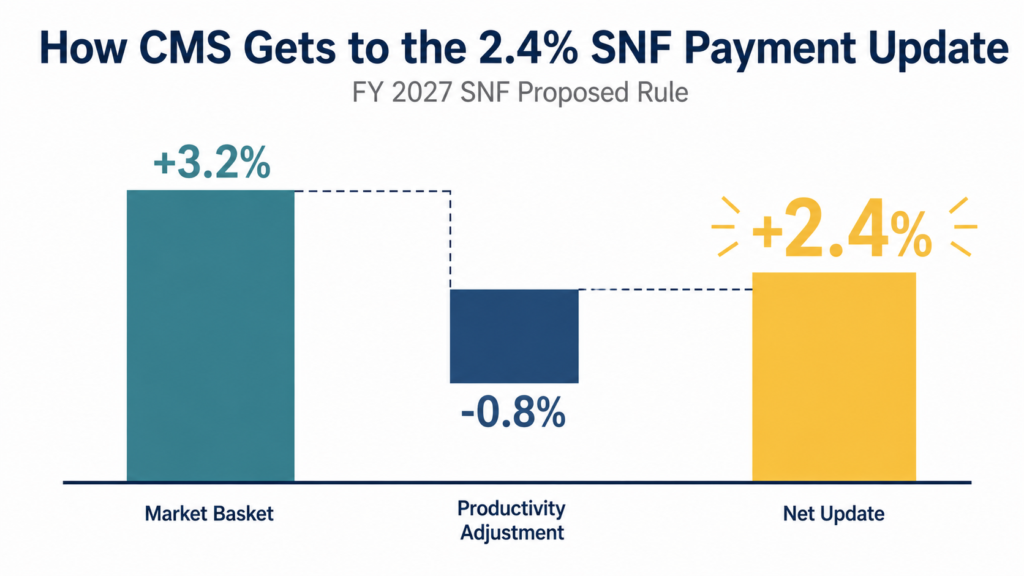
FY 2027 SNF Proposed Rule Payment Update: 2.4%
The headline number in the FY 2027 SNF proposed rule is the proposed 2.4% payment update.
CMS states that this reflects a proposed 3.2% SNF market basket increase, reduced by a 0.8% productivity adjustment. CMS estimates this would increase Medicare payments to SNFs by approximately $888 million in FY 2027, before accounting for certain SNF Value-Based Purchasing reductions.
For many skilled nursing operators, the concern is obvious.
A 2.4% increase may be better than a decrease, but it does not necessarily reflect the cost reality inside today’s facilities. Labor, clinical supplies, insurance, agency staffing pressure, technology, food, and general operating expenses have continued to rise.
That makes the payment update an advocacy issue.
Operators should be prepared to show CMS what their actual cost increases look like. General frustration is not enough. Facility-level data is much stronger.
If your costs have increased beyond 2.4%, your comments should make that clear.
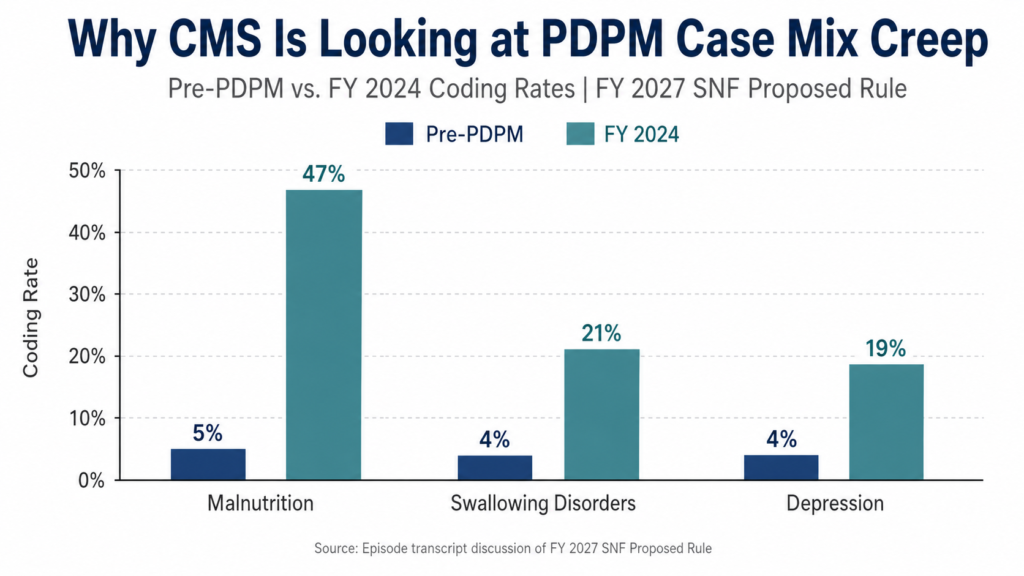
PDPM Case Mix Creep in the FY 2027 SNF Proposed Rule
The most important part of the FY 2027 SNF PPS proposed rule may be the discussion around PDPM case mix.
CMS is requesting information on observations and analysis related to the Patient Driven Payment Model, including case mix intensity changes under PDPM. Industry summaries of the rule have also highlighted CMS’s focus on PDPM trends and possible future adjustments.
This matters because CMS is not simply looking at payment levels.
CMS is looking at whether the coding patterns under PDPM match the actual clinical complexity and resource utilization of SNF residents.
That should get every operator’s attention.
If CMS believes that case mix intensity has increased faster than clinical complexity or resource needs, future payment adjustments could follow. Even if no immediate PDPM overhaul is finalized in this rule, the direction is clear: CMS is watching.
For skilled nursing leaders, the takeaway is simple.
You need to know whether your MDS coding is accurate, defensible, and supported by documentation.
Why MDS Accuracy Is Becoming a Strategic Priority
The FY 2027 SNF proposed rule should push MDS accuracy higher on the executive priority list.
This is not just an MDS department issue. It is a reimbursement issue, a compliance issue, a clinical documentation issue, and an operational risk issue.
If your facility is capturing depression, swallowing disorders, malnutrition, speech needs, nursing complexity, or NTA conditions, the question is not simply whether those items are coded.
The question is whether they are supported.
Can your documentation prove the condition exists?
Can your team show that the interview was completed correctly?
Can your therapy documentation support the services being delivered?
Can your nursing documentation support the clinical picture reflected on the MDS?
This is where many facilities become vulnerable.
Under PDPM, accurate coding can create appropriate reimbursement. But unsupported coding can create audit risk, denials, takebacks, and future payment pressure across the industry.
That is why now is the time for a SNF MDS audit, not after CMS finalizes future changes.
Therapy, PDPM, and the Risk of Future Rebalancing
The rule also raises concerns around how CMS may view therapy costs and component-level payment accuracy under PDPM.
According to the episode discussion, CMS data suggests that certain per diem costs for therapy and NTA components have declined, while case mix intensity has increased in several categories. Melissa Brown specifically highlighted the concern that future adjustments could create winners and losers across PDPM components, especially if CMS attempts to “right size” payment based on its interpretation of cost and utilization trends.
For operators, the danger is not theoretical.
If CMS eventually reduces components tied to Speech, Nursing, or NTA, the impact could be significant. Many SNFs already rely on Medicare reimbursement to help offset pressure from Medicaid, Medicare Advantage, and other lower-margin payer sources.
A meaningful reduction to core PDPM components could force difficult decisions around staffing, clinical programs, therapy delivery, and overall operations.
This is why operators should not wait passively for the final rule.
They should model the potential impact now.
Ask:
How would a component-level adjustment affect our building?
What would happen if Nursing, Speech, or NTA reimbursement declined?
Are we over-reliant on any one component?
Do our coded conditions match our documentation?
Do our therapy patterns support the clinical needs of our residents?
If you cannot answer those questions confidently, the proposed rule is a warning sign.
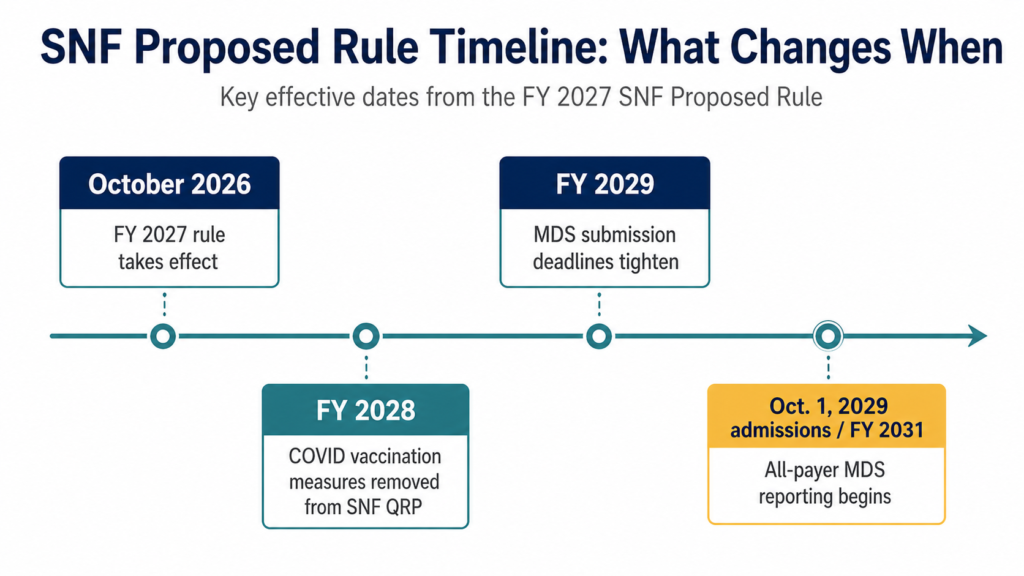
All-Payer MDS Reporting in the FY 2027 SNF Proposed Rule
Another major provision in the FY 2027 SNF proposed rule involves expanded MDS reporting.
CMS is proposing to require submission of MDS data for each resident receiving covered skilled care in a SNF, regardless of payer. The proposed rule also includes updates to SNF QRP data submission deadlines and other reporting requirements.
This is a major shift, even if the operational burden is not equal for every facility.
Many managed care payers already require MDS completion in practice. For those facilities, the additional workload may be modest. But the broader implication is much bigger.
CMS wants more complete visibility into skilled nursing performance across payer types.
That matters because Medicare fee-for-service is no longer the whole picture. As Medicare Advantage enrollment continues to grow, quality performance based only on traditional Medicare patients becomes less representative of the full resident population.
All-payer MDS reporting could eventually make quality performance more visible across Medicare Advantage, Medicaid, commercial insurance, and other payer sources.
For operators, this means quality strategy can no longer live in a Medicare-only silo.
Medicare Advantage Quality Performance Needs More Attention
The FY 2027 SNF proposed rule points toward a future where quality performance may become more visible across payer types.
That should concern operators who have never compared Medicare fee-for-service quality performance against Medicare Advantage quality performance.
Many facilities know how they perform under traditional Medicare measures. Fewer have a clear picture of how their managed care population compares.
That gap matters.
If Medicare Advantage outcomes are weaker, inconsistent, or poorly documented, that may become a larger problem as all-payer reporting expands.
Operators should begin reviewing:
- Medicare vs. Medicare Advantage discharge outcomes
- Functional improvement patterns by payer
- Documentation consistency by payer
- Therapy utilization by payer
- MDS completion processes across payer types
- Hospital readmission patterns
- Quality measure performance by population
This is not just about compliance. It is about understanding whether your facility is delivering consistent clinical outcomes across the full census.
What Skilled Nursing Operators Should Do Now
The SNF proposed rule 2027 should not sit in a folder until the final rule is published.
Operators should act now in five key areas.
1. Submit comments to CMS
Comments on the proposed rule are due by June 1, 2026.
If you operate skilled nursing facilities, you should consider submitting comments, especially around payment adequacy, PDPM case mix concerns, and the potential impact of future component-level adjustments.
The strongest comments will include data.
Show your cost increases.
Show your therapy utilization.
Show your nursing cost pressures.
Show the operational impact of proposed or potential cuts.
CMS needs to hear what these changes mean at the facility level.
2. Audit your MDS coding
This is one of the most important steps.
Review your coding patterns for depression, swallowing disorders, malnutrition, speech-related conditions, nursing complexity, and NTA comorbidities.
Look for outliers.
Compare your rates to internal history, peer benchmarks, and national trends when available.
Most importantly, verify that coded items are supported by documentation.
A SNF MDS audit can help identify both missed reimbursement opportunities and areas of risk.
3. Review therapy documentation and utilization
CMS is paying attention to resource utilization under PDPM.
That means therapy documentation needs to be clear, clinically appropriate, and tied to resident need.
Operators should evaluate whether therapy delivery patterns align with acuity, outcomes, and documentation.
If your therapy program is underdelivering, overgeneralizing, or failing to clearly connect services to resident need, now is the time to fix it.
4. Model the financial impact
Do not wait for the final rule to understand the possible impact.
Model different case mix adjustment scenarios.
What happens if certain PDPM components are reduced?
What happens if payment updates fall below cost growth?
What happens if Medicare Advantage continues to grow while traditional Medicare becomes a smaller share of your skilled census?
A clear financial model gives leadership a better foundation for advocacy and operational planning.
5. Compare Medicare and Medicare Advantage quality performance
All-payer MDS reporting points toward a future where operators need a better understanding of quality across payer types.
Start now.
Compare Medicare fee-for-service and Medicare Advantage outcomes. Look for documentation gaps, therapy differences, discharge patterns, and quality measure variation.
If Medicare Advantage performance is weaker, do not wait until that data becomes more visible.
The Bottom Line
The FY 2027 SNF proposed rule is more than a routine annual payment update.
Yes, the proposed 2.4% increase matters. But the bigger message is that CMS is looking closely at PDPM case mix intensity, MDS data, documentation quality, and broader reporting across payer sources.
For skilled nursing operators, this is the moment to get ahead of the issue.
Audit your MDS coding.
Review your documentation.
Model your reimbursement risk.
Compare your quality performance by payer.
And submit comments that show CMS what is actually happening inside your facility.
Because the facilities that prepare now will be in a much stronger position when future payment, quality, and reporting changes become final.
Need Help Reviewing Your MDS, PDPM, or Reimbursement Strategy?
Gravity Consulting helps skilled nursing and senior living providers improve reimbursement accuracy, strengthen MDS documentation, evaluate therapy performance, and identify operational opportunities before they become financial problems.
If you are unsure whether your MDS coding, PDPM strategy, or documentation can stand up to increased scrutiny, now is the time to take a closer look.
You can also listen to the full episode of Gravity Healthcare Hacks with Melissa Brown for a deeper discussion of the FY 2027 SNF proposed rule and what operators should be watching next.