Nursing home risk management rarely turns on one bad moment. The greater risk is when a fall, wound, medication issue, or change in condition becomes evidence of a larger operational pattern: understaffing, incomplete documentation, ignored alerts, weak follow-through, or a gap between resident acuity and the resources assigned to care for that population.
That is the risk senior living and skilled nursing executives cannot afford to miss.
In a recent episode of Senior Living Executive Strategy, Melissa Brown spoke with Rob Schenk of Schenk Nursing Home Abuse Law about what plaintiff’s attorneys look for when evaluating nursing home claims. The conversation was not just about litigation. It was about nursing home risk management at the operational level.
Because in today’s environment, the legal question is rarely limited to, “Did something happen?”
The stronger question is, “What does the record show the organization knew, and what did leadership do about it?”
Nursing Home Risk Management Now Starts With Staffing Data
Staffing has always been central to quality in skilled nursing. What has changed is how visible staffing has become.
CMS Payroll-Based Journal data gives the public a facility-level view of nursing staff hours, staff categories, and census. That means staffing patterns are no longer buried inside a schedule or payroll report. They can be reviewed by surveyors, plaintiff’s attorneys, referral partners, families, lenders, buyers, and competitors.
That visibility matters.
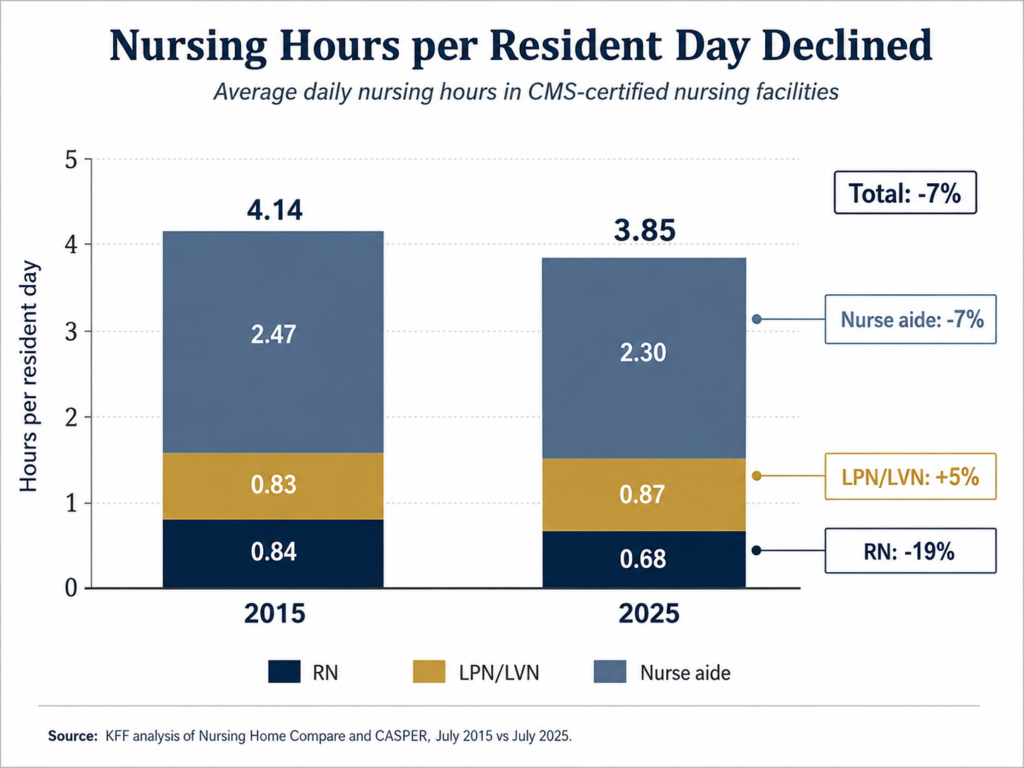
KFF reported that, as of July 2025, there were 14,742 CMS-certified nursing facilities with about 1.24 million residents. Those residents received an average of 3.85 nursing hours per resident day, including RN, LPN/LVN, and nurse aide hours. Between July 2015 and July 2025, total nursing hours per resident day declined 7%. RN hours declined 19%.
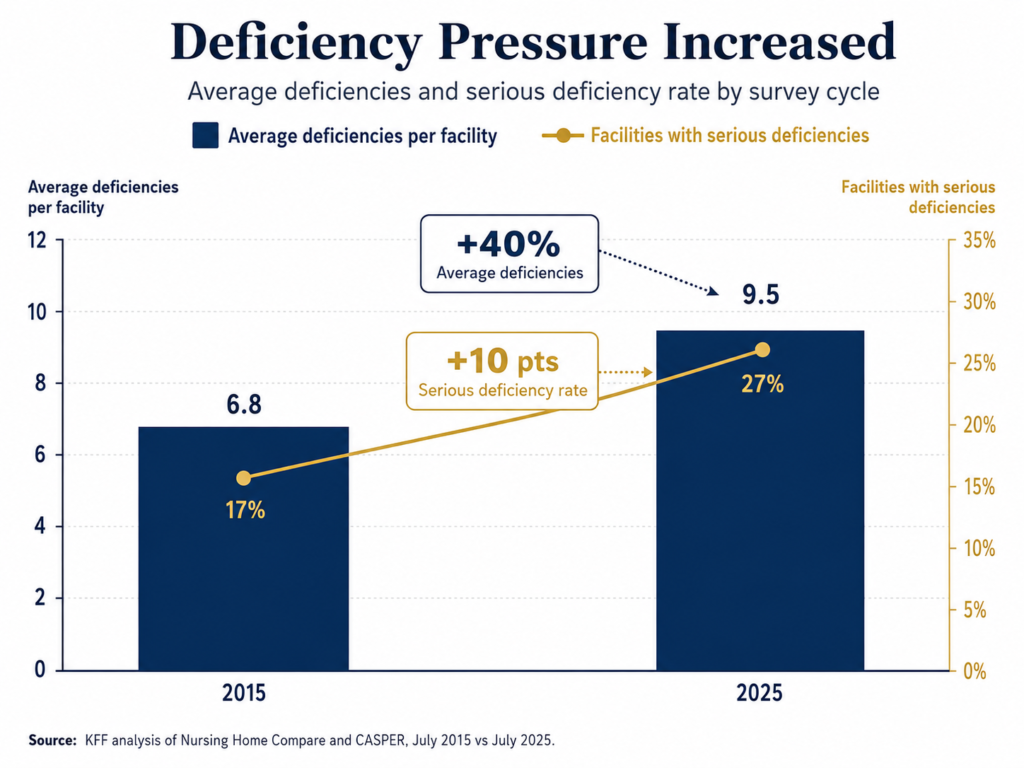
During that same period, survey deficiencies increased. The average number of deficiencies per nursing facility rose from 6.8 to 9.5, a 40% increase. The share of facilities with serious deficiencies, meaning actual harm or immediate jeopardy, rose from 17% to 27%.
Those numbers do not prove that every facility is unsafe. They do show why staffing is becoming a more important risk signal.
For executives, the issue is not simply whether a building can point to a minimum requirement and say, “We met it.”
The better question is whether staffing matches the acuity of the residents in the building.
Minimum staffing is not the same as appropriate staffing
A facility can meet a technical staffing minimum and still be exposed if the resident population requires more care than the staffing model can reasonably support.
That distinction matters because resident acuity is not static.
If a building is admitting more complex residents, managing more wounds, seeing greater behavioral health needs, caring for residents with higher ADL dependency, or capturing higher CMI through more accurate documentation, the operating model has to adjust.
This is where providers can unintentionally create risk.
They improve documentation.
They capture acuity more accurately.
They increase PDPM or Medicaid reimbursement.
Their CMI rises.
But their staffing model, care planning process, and clinical oversight stay the same.
From a reimbursement perspective, higher CMI may be appropriate and financially necessary. From a legal and survey perspective, it can also become evidence that the facility knew its population required more care.
The answer is not to under-document acuity. That would create a different and potentially larger problem.
The answer is to connect reimbursement accuracy to operational reality.
When Gravity works with providers on PDPM and Medicaid accuracy, the opportunity is often significant. Gravity has seen organizations increase reimbursement by $10 to $40 per patient day through better documentation accuracy and care coordination. For a 100-bed skilled nursing facility at 85% occupancy, that represents roughly $310,000 to $1.24 million in annualized reimbursement opportunity.
But the strongest operators do not stop at the revenue number.
They ask what that acuity data means for staffing, resident risk, wound prevention, fall prevention, restorative programming, therapy utilization, care planning, clinical supervision, and documentation follow-through.
That is why nursing home risk management has to connect acuity, reimbursement, staffing, and clinical follow-through instead of treating them as separate issues.
That is the difference between capturing revenue and building a more defensible operation.
Documentation Is a Nursing Home Risk Management Issue
The phrase “if it was not documented, it was not done” may feel overused, but it remains one of the most practical risk management truths in long-term care.
The record is what survives after the shift is over.
If a resident develops a pressure injury, falls, experiences a decline, misses a medication, requires transfer, or has a change in condition, the organization needs to be able to show what happened.
What was assessed?
Who was notified?
What changed in the care plan?
Was the family contacted?
Was the physician notified?
Were interventions implemented?
Was follow-up completed?
Did the next shift know what needed to happen?
When documentation is incomplete, the organization may have done more than the record shows. But outside reviewers do not get to see good intentions. They see the chart.
That is why documentation gaps can become so damaging. They allow someone else to write the story.
Maybe the resident was admitted with a wound, but present-on-admission documentation was incomplete. Maybe staff were turning and repositioning, but the record is inconsistent. Maybe a fall risk was known, but interventions were not updated. Maybe vitals were abnormal across several shifts, but there is no clear escalation trail.
Each gap may seem explainable in isolation. Together, they can start to look like a system that was not paying attention.
Technology can reduce burden, but it can also sharpen the record
AI documentation tools, transcription platforms, EHR alerts, and automated workflows can help clinical teams work more efficiently. Used well, they can reduce missed documentation, improve consistency, and make risk easier to identify.
Used poorly, they can create a clearer audit trail of missed opportunities.
If an EHR generates repeated alerts for abnormal vitals, medication risk, skin changes, fall risk, late documentation, or missed follow-up, the question becomes whether the team responded or simply clicked through.
That is a very different issue than whether a note contains a typo.
The deeper risk is that the technology shows the warning signs were there, but the organization did not act on them.
Providers should be auditing how their systems are actually being used. That includes alert overrides, late entries, unsigned notes, copied-forward language, high-risk resident documentation, wound documentation, fall follow-up, and change-in-condition workflows.
Technology should make care more reliable. It should not become an expensive way to document that the same warnings were ignored multiple times.
In a modern nursing home risk management strategy, technology should make clinical risk easier to see, not easier to ignore.
The cost of risk is already showing up in the data
Liability is not theoretical in senior living and long-term care.
Marsh’s 2024 General and Professional Liability Benchmark Report reviewed nearly 10,300 closed claims across senior living and long-term care, representing approximately $1.87 billion in paid indemnity and expense over ten years. The report identified falls as the primary loss driver for both senior living and long-term care, with wounds as the second primary loss driver for long-term care.
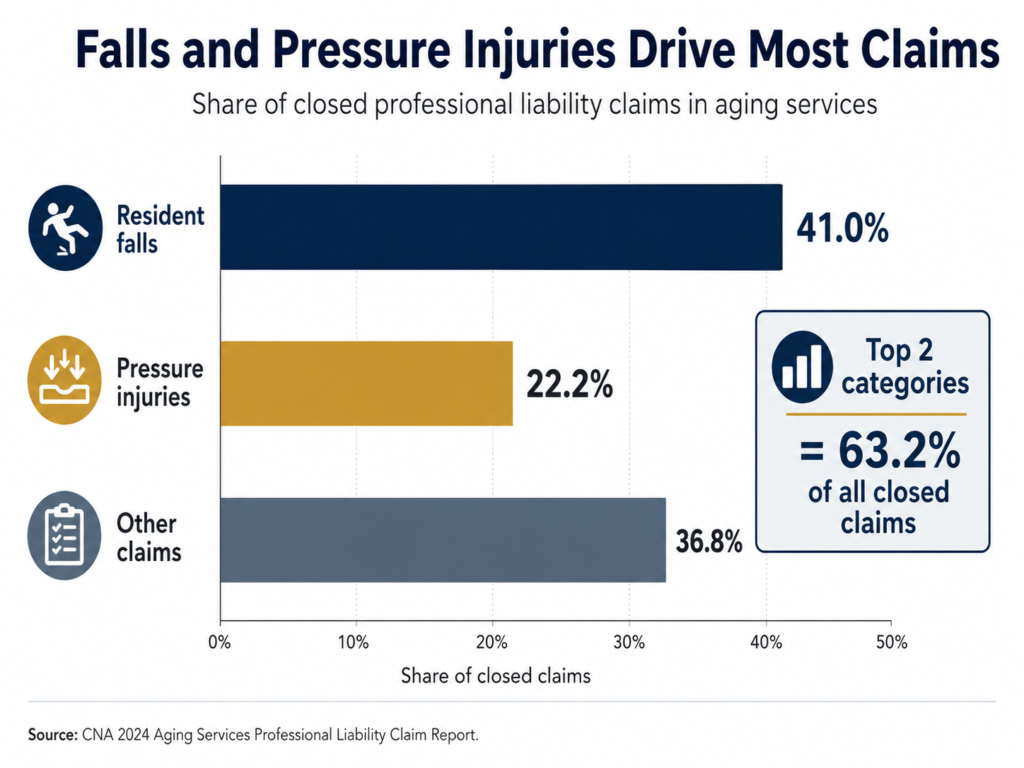
CNA’s 2024 Aging Services Professional Liability Claim Report found that falls accounted for 41.0% of all closed claims, while pressure injuries accounted for another 22.2%. Together, those two categories represented 63.2% of all closed claims in the dataset.
The severity is equally important. CNA reported an average total incurred of $259,443 across all facilities, with several high-severity allegations exceeding $300,000 on average, including resident abuse, failure to move a resident to a higher level of care, failure to follow physician orders, medication errors, and elopement.
Those categories are not random.
They usually connect back to core operating systems: staffing, supervision, documentation, care planning, communication, follow-up, training, and leadership accountability.
When those systems are weak, risk becomes more expensive. When they are strong, the building becomes easier to manage, easier to survey, easier to defend, and easier to improve.
The real opportunity is to manage performance and risk together
Too many providers still treat reimbursement, staffing, documentation, quality, survey readiness, and legal exposure as separate issues.
Inside the building, they are connected.
The MDS process affects reimbursement and reflects acuity. Acuity should influence staffing and care planning. Staffing affects outcomes and documentation completion. Documentation affects survey readiness and legal defensibility. Survey outcomes affect star ratings, referrals, census, payer relationships, and reputation.
A breakdown in one area eventually shows up somewhere else.
That is why the best operators do not wait for a lawsuit, complaint survey, poor star rating, or family escalation to find out where the system is weak. They look for the gaps while there is still time to fix them.
Gravity helps providers do that by looking across the full operating picture, including MDS accuracy, PDPM and Medicaid reimbursement, staffing alignment, documentation quality, mock survey readiness, clinical follow-through, therapy performance, interim leadership, and operational turnaround.
The value is not just finding problems. It is connecting the problems to the numbers.
If PDPM accuracy is off, the building may be leaving $10 to $40 per patient day on the table.
If acuity is rising but staffing has not been reassessed, the building may be increasing its risk exposure without realizing it.
If documentation is incomplete, the building may be weakening its survey position and legal defense even when care was provided.
If quality systems are not disciplined, the building may be carrying avoidable star rating drag, census pressure, referral concerns, and reputational risk.
And if leadership does not have visibility into these issues, the organization is managing by reaction instead of control.
The Nursing Home Risk Management Question for Executives
The most important question for senior living and skilled nursing leaders is not, “Are we perfect?”
No provider is.
The better question is:
If someone outside the organization reviewed our staffing data, documentation, acuity trends, alert patterns, care plans, survey history, and outcomes, what story would those records tell?
Would they show a provider that understood its risks and acted on them?
Or would they show a provider where the warning signs were visible, but the system did not respond?
That is the difference between an unfortunate incident and a larger operational narrative.
And in today’s environment, that narrative matters.
Senior living and skilled nursing leaders do not need more fear. They need better visibility, stronger systems, and a clearer connection between clinical operations, reimbursement, staffing, documentation, and risk.
That is where Gravity helps.
Gravity Consulting is an outcomes-focused consulting firm for senior living, skilled nursing, and home health organizations. If your organization has an operational, clinical, reimbursement, staffing, documentation, or growth issue that needs to be solved, start the conversation to learn how Gravity can help.